Why one generalist medical model spreads itself too thin - and how giving each clinical department its own curated AI brain, then letting those brains consult one another, surfaces problems earlier, more consistently, and with fewer false alarms.
The Problem Is Not Too Little Data. It Is Too Much.
Modern medicine generates an overwhelming volume of data. A single patient encounter can produce lab results, imaging studies, vital signs, clinical notes, genetic markers, and historical records. The challenge facing healthcare systems is not a shortage of information but the difficulty of synthesizing it quickly enough to identify problems before they escalate.
A promising architectural response is the deployment of curated, domain-specific AI models that serve as the "brain" for individual agents dedicated to each medical department. Rather than relying on a single generalist model attempting to cover all of medicine, this approach assigns each department its own purpose-built intelligence, trained and refined on the data, terminology, and reasoning patterns specific to that specialty.
This article examines how this departmental-agent architecture works, why curation matters, and the concrete mechanisms by which it enables faster and more accurate identification of medical problems.
Designing clinical AI for your health system? Book a free 30-minute architecture review and we will walk through a departmental-agent design with one of our engineers.
The Core Concept: One Brain Per Department
In a departmental-agent architecture, each clinical department - cardiology, radiology, oncology, neurology, nephrology, emergency medicine, pathology, and so on - is paired with a dedicated AI agent. The "brain" of each agent is a curated model: a model whose training data, fine-tuning, knowledge base, and decision logic have been deliberately shaped around the needs of that single specialty.
The contrast is with a monolithic generalist system. A general-purpose medical model must spread its capacity across the entire breadth of medicine, which dilutes its depth in any one area and forces it to navigate enormous semantic ambiguity. The word "mass" means something different to a radiologist than to a physicist. "Block" means something specific in cardiology (heart block) versus anesthesiology (nerve block). A curated cardiology model encounters "block" almost exclusively in its cardiac sense, so its interpretations are sharper and its error rate on domain-specific reasoning is lower.
The departmental brain is not merely a filtered version of a general model. It is curated along several dimensions simultaneously: the corpus it learns from, the clinical guidelines it encodes, the reference ranges and thresholds it applies, the diagnostic decision trees it follows, and the tools and databases it can query.
What "Curation" Actually Means
Curation is the deliberate, ongoing process of shaping a model to match the realities of a specific clinical domain. It works across several layers.
Data Curation
Data curation ensures the model learns from high-quality, representative, and correctly labeled examples from the department. A radiology brain is trained on imaging studies paired with confirmed diagnoses and radiologist reports, with careful attention to image quality, modality, and the prevalence of conditions. Mislabeled or low-quality data is filtered out, and rare-but-critical conditions are deliberately oversampled so the model does not overlook them simply because they are uncommon.
Knowledge Curation
Knowledge curation encodes the authoritative guidelines, protocols, and reference standards of the specialty. A cardiology brain incorporates current guidelines for managing acute coronary syndrome, heart failure staging, and arrhythmia classification. Because these guidelines are explicitly curated rather than absorbed implicitly, they can be updated when professional bodies revise their recommendations, keeping the agent current.
Threshold and Context Curation
Threshold and context curation tunes the model to the population it serves. Reference ranges for laboratory values, risk scores, and alert thresholds differ across specialties and patient populations. A nephrology brain interprets creatinine and glomerular filtration rates against the nuanced baselines relevant to kidney disease staging, while a pediatric department's agents apply age-adjusted norms that would be inappropriate for adults.
Tool Curation
Tool curation equips each agent with access to the specific calculators, databases, imaging systems, and decision-support resources its specialty relies on. An oncology brain can query tumor staging systems and molecular databases. An infectious disease brain can access antimicrobial resistance patterns and local epidemiological data.
How Departmental Agents Accelerate Problem Identification
Reduced Search Space and Faster Reasoning
A specialist agent operates within a constrained, well-defined problem space. When a curated cardiology brain evaluates a patient, it is not weighing the probability of obscure neurological or dermatological conditions. It focuses its reasoning on the differential diagnoses relevant to cardiac presentations. This narrowing dramatically reduces the computational and cognitive search space, allowing the agent to reach high-confidence conclusions faster. The agent can rapidly rank likely diagnoses, flag the most dangerous possibilities, and recommend confirmatory tests without being distracted by improbable alternatives.
Higher Sensitivity to Subtle, Specialty-Specific Signals
Because the curated brain has seen vast numbers of examples within its narrow domain, it becomes exquisitely sensitive to subtle patterns that a generalist might miss. A radiology agent trained intensively on chest imaging can detect early, faint signs of conditions - a small nodule, an early interstitial pattern, a subtle effusion - that are easy to overlook. This heightened sensitivity translates directly into earlier identification of problems, often at a stage when intervention is most effective.
Continuous Monitoring and Early Alerting
Departmental agents can run continuously against streams of incoming data, monitoring patients in real time. An emergency medicine agent can watch vital sign trends and lab results as they arrive, raising an alert the moment a pattern consistent with sepsis, hemorrhage, or cardiac deterioration emerges. Because the agent is specialized, its alerts are more precise and carry fewer false alarms, which combats the alert fatigue that plagues less-targeted systems.
Consistency and Tireless Vigilance
Human clinicians are subject to fatigue, cognitive load, and variability. A curated departmental brain applies the same rigorous reasoning to the first patient of the day and the last, at three in the morning as at noon. This consistency means that the quality of problem identification does not degrade under pressure, and that no case receives a cursory review simply because the department is overwhelmed.
Coordination Across Departments
The power of this architecture is amplified when departmental agents coordinate. Many serious medical problems do not respect departmental boundaries. A patient presenting to the emergency department with shortness of breath might have a cardiac, pulmonary, renal, or hematologic cause. In a coordinated multi-agent system, the emergency agent can consult the cardiology, pulmonology, and nephrology brains, each contributing its specialized assessment. An orchestration layer synthesizes these inputs, surfacing a unified differential that benefits from deep expertise in every relevant domain simultaneously.
This mirrors how a hospital actually works - through consultation between specialists - but compresses the timeline from hours or days to seconds. A condition that might otherwise be identified only after sequential referrals can be flagged in a single coordinated pass. Cross-departmental agents are particularly valuable for catching conditions that fall in the gaps between specialties, where each individual department might assume the problem belongs to another.
Architectural Considerations
A robust departmental-agent system requires careful design beyond the models themselves. The diagram below shows how the pieces fit together - from raw data sources, through a shared patient context and orchestration layer, out to the curated departmental brains, and back to the clinician who stays in control.
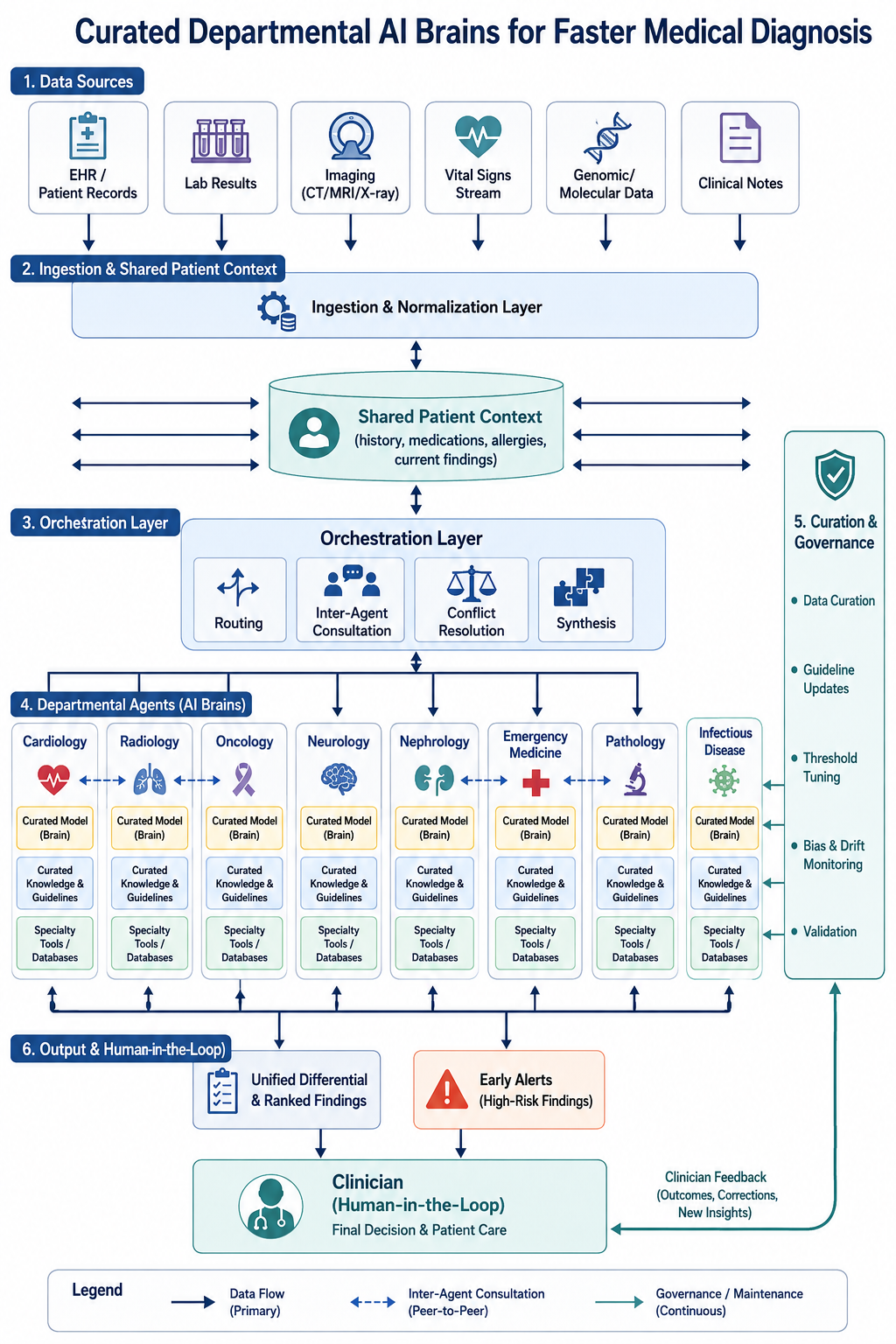
An orchestration layer routes patient data to the appropriate agents, manages consultations between them, and resolves conflicts when agents disagree. When the cardiology and pulmonology brains offer competing explanations, the orchestrator must present both with their supporting evidence rather than arbitrarily choosing one.
A shared patient context ensures that every agent works from the same complete and current picture of the patient, including history, current medications, allergies, and the findings already contributed by other agents. Fragmented context would undermine the benefits of coordination.
A human-in-the-loop design keeps clinicians firmly in control. The agents accelerate and support identification, but the responsibility for diagnosis and treatment remains with qualified medical professionals. The system should make its reasoning transparent, citing the data and guidelines behind each conclusion so clinicians can verify and trust its outputs.
A governance and updating mechanism maintains each curated brain over time, incorporating new guidelines, retraining on new data, monitoring for performance drift, and auditing for bias across patient populations.
Benefits Beyond Speed
While faster identification is the headline benefit, the architecture offers more.
- Easier to validate and certify. Narrow scope makes each brain's behavior more predictable and testable.
- Easier to update. A change in cardiology guidelines requires modifying only the cardiology brain, not retraining an entire monolithic system.
- More explainable. Each brain reasons within a coherent specialty framework, which is essential for clinical trust and regulatory approval.
- Distributed risk. A problem in one departmental brain does not compromise the entire system.
Challenges and Cautions
This approach is not without difficulties. Curating and maintaining many specialized models demands significant resources and sustained expert involvement. Coordination between agents introduces complexity and potential failure points. Boundary cases - conditions that genuinely span specialties - require careful handling to avoid being dropped between agents. Data quality, privacy, and security must be rigorously protected throughout. And every agent must be continuously validated against real-world outcomes to ensure it is helping rather than introducing subtle errors or biases.
Critically, these systems must augment rather than replace clinical judgment. Their value lies in surfacing possibilities faster and more consistently, giving clinicians more time and better information, not in removing human accountability from medicine.
Conclusion
Curated models serving as the brain for departmental agents represent a thoughtful response to the central challenge of modern medicine: extracting timely insight from overwhelming data. By giving each specialty a dedicated, deeply tuned intelligence - and by enabling those intelligences to consult one another - healthcare systems can identify medical problems earlier, more consistently, and with greater precision than either generalist systems or overstretched human teams working in isolation.
The architecture aligns naturally with how medicine is already organized, amplifying the strengths of specialization while using coordination to overcome its traditional weakness of siloed thinking. Implemented carefully, with humans firmly in the loop and rigorous governance in place, this approach offers a credible path toward faster, safer, and more effective diagnosis.
Building clinical AI that doctors can trust? Talk to TunerLabs - we engineer production multi-agent systems, including curated domain-specific models and the orchestration layers that let them work together. From a single departmental brain to a coordinated cross-specialty system, we design architectures that surface problems earlier and keep humans firmly in the loop.
Topics:
Master Claude Code
The complete architecture guide — Skills, Agents, Memory & the full Tools reference. Everything in one beautiful page.